TW Child Dental Consent Form
CDBS Medicare
Childcare/Kindigarten Details
If Child Attends School:
Parent/Guardian Info
Medical History
Oral Hygiene & Habits
Media consent for awareness and education
Dental treatment consent
Note: Only essential treatment will be provided during visits.
A written summary will be sent home after each appointment.
For any urgent issues, you will be contacted immediately.
Patient's/Child Details
About this Program
The Child Dental Benefits Schedule (CDBS) is an Australian Government program that provides access to basic dental services, within a benefit cap, over a relevant two calendar year period.
For more info please visit this link:
https://www.humanservices.gov.au/health-professionals/services/child-dental-benefits-schedule/
Privacy and Consent Information.
Your personal information is protected by law, including the Privacy Act 1988 and the Australian Privacy Principles (APPs), and is being collected by your Dental Provider on behalf of the Department of Health, Disability and Aging (the Department), for the primary purpose of facilitating basic dental services under the Child Dental Benefits Schedule.
If you do not provide this information, services will not be able to be provided to you under the CDBS.
By providing your personal information to your Dental Provider, you consent to the department collecting this personal information about you from your Dental Provider.
You can access the Department's APP privacy policy at https://www.health.gov.au/resources/publications/privacy-policy.
The Department can be contacted by telephone on (02) 6289 1555 or via email at [email protected].
The Department will not disclose your personal information to any overseas recipients.
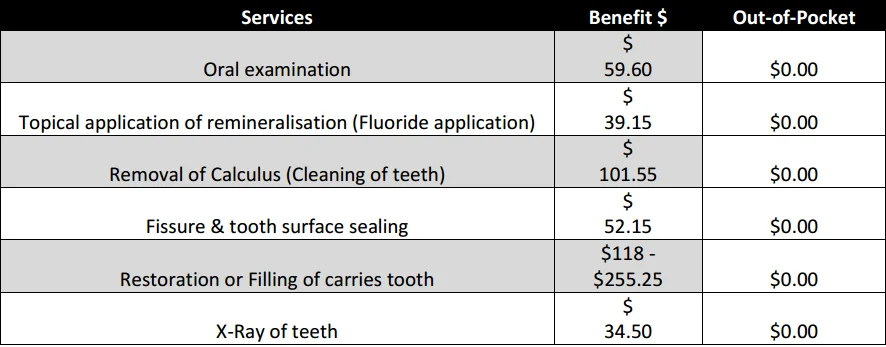
All services listed below (except for the oral examination) will be provided only if required.
Consent & Agreement
I, the patient/parent/legal guardian, certify that I have been informed:
of the treatment that has been or will be provided from this date under the Child Dental Benefits Schedule and the likely cost of this treatment.
that I will be bulk billed for services under the Child Dental Benefits Schedule.
that there will be no out-of-pocket costs for dental services provided within a public clinic; and
that benefits for some services may have restrictions, and
that the Child Dental Benefits Schedule covers a limited range of dental services.
This form is valid up to 31st December of the calendar year for which it is signed.
By completing and signing this form, I confirm the following:
I am the legal parent or guardian of the child listed above.
I have read and understood the nature of the dental services being offered.
I authorize Tooth Wagon to provide necessary dental care under the CDBS or as a private service if not eligible.
I give consent for my child to attend the mobile dental clinic supervised by school or child care staff.
I acknowledge this consent remains valid for up to two visits within the current calendar year.
I affirm all information provided is accurate and up-to-date.